June 2026
 Download PDF Format
Download PDF Format
Information sheet
Voluntary Incident Reporting
Exposure and non-exposure incidents involving human pathogens and toxins (HPTs) that are not mandated under the Human Pathogens and Toxins Act (HPTA) and its Regulations (HPTR) can be submitted to the Public Health Agency of Canada voluntarily. These incidents are summarized below.
What constitutes a voluntary report?
Incidents not mandated under the HPTA and HPTR include:
- Incidents involving Risk Group (RG) 1 pathogens
- Exposures or laboratory-acquired infections involving pathogens/toxins in their natural environment or primary samples (e.g. blood, serum, saliva, milk, urine; not cultured or processed)
- Incidents occurring in facilities exempt from licence requirements
Results
213 voluntary laboratory incidents reported:
- 139 exposure reports (including 1 suspected and 1 confirmed laboratory-acquired infection [LAI] and 16 ruled out cases)
- 74 non-exposure reports (including 56 inadvertent possessions/productions, 13 inadvertent releases, 3 stolen biological agents, 1 missing or lost biological agent and 1 security sensitive biological agent (SSBA) not received within 24 hours of expected arrival)
Main Activities
The most common activity at the time of an exposure incident was microbiology (43.9%). For non-exposure incidents, identification microbiology activities were most common (39.7%).
Sectors
66 exposure incidents were reported from the hospital sector (47.5%) and 32 from the academic sector (23.0%).
39 non-exposure incidents were reported from the hospital sector (53.4%) and 13 from both the academic and private sector (17.8% each).
Root causes of exposure
From a total of 264 root causes citations, the most common were human factors (26.5%), standard operating procedures (18.2%) and training (15.2%). This mirrors the top cited root causes in mandatory exposure reports in 2025.
Occurrence types
181 occurrence types were identified in exposure incidents.
The most common occurrence types were related to procedures (23.8%), spills (14.9%) and other (20.4%) occurrence types involving inadvertent possession.
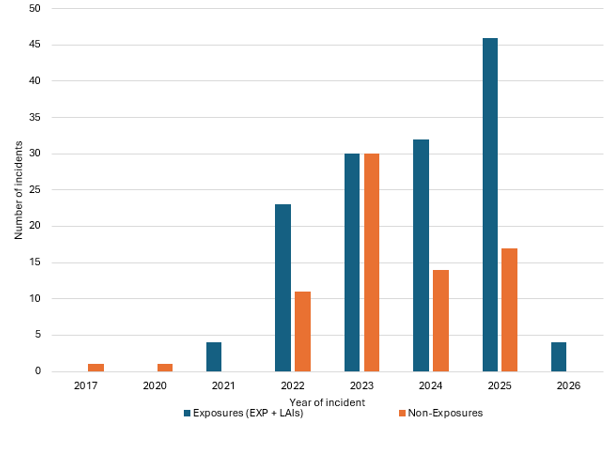
Note: Facilities have been able to report voluntarily since November 2021. Incidents dated before 2021 were retroactively reported.
Affected persons (N=306)
An average of 2.20 people were affected per exposure incident. Most were technologists/ technicians (n=249; 81.4%) and exposed via inhalation (n=159; 52.0%).
Implicated pathogens
In Exposure incidents
There were 104 known HPTs and 46 unknown HPTs implicated.
- 75 HPTs (50%) were non-SSBAs. Of these, 14 (9.3%) were RG1, 36 (24.0%) were RG2 and 25 (16.7%) were RG3.
- 29 HPTs (19.3%) were SSBAs which were all RG3.
- The most implicated agent type in RG1 HPTs were cell lines (2.7%) and bacteria (2.0%).
- The most implicated agent types in RG2 HPTs were bacteria (14.7%) and viruses (6.0%).
- The most implicated agent types in RG3 HPTs were bacteria (17.3%), prions and viruses (7.3% each).
The most common pathogens were Neisseria meningitidis (8.7%) and Creutzfeldt-jakob disease agent (7.3%).
In Non-Exposure incidents
There were 92 known HPTs and 17 unknown HPTs implicated.
- 76 HPTs (69.7%) were non-SSBAs. Of these, 15 (13.8%) were RG1, 31 (28.4%) were RG2 and 29 (26.6%) were RG3.
- 16 HPTs (14.7%) were SSBAs. Of these, 15 (13.8%) were RG3 and 1 (0.9%) was RG4.
- The most implicated agent type in RG1 HPTs was bacteria (11.9%).
- The most implicated agent types in RG2 HPTs were bacteria (19.3%) and fungi (3.7%).
- The most implicated agent types in RG3 HPTs were bacteria (14.7%) and fungi (13.8%).
- The RG4 was a virus.
The most common pathogens were Mycobacterium tuberculosis (9.2%) and Creutzfeldt-jakob disease agent (6.4%).
Comparison: Voluntary and mandatory incident reports
Similarities were found between the most cited main activity, sector, root cause, occurrence type, affected person’s role and route of exposure in voluntary and mandatory incident reports. A greater proportion of RG3 pathogens were implicated in the voluntary incidents compared to the mandatory incidents because they were related to primary samples or pathogens unknown at the time of the exposure during diagnostic activities.
Why is voluntary reporting important?
Voluntary reporting allows a broader range of incidents to be captured, including events outside regulatory requirements that might otherwise go unreported. By sharing these experiences, facilities contribute to a more complete understanding of biosafety risks and help inform the Public Health Agency of Canada’s targeted prevention strategies.
Contact PHAC at biosafety-biosecurite@phac-aspc.gc.ca if you have more questions.